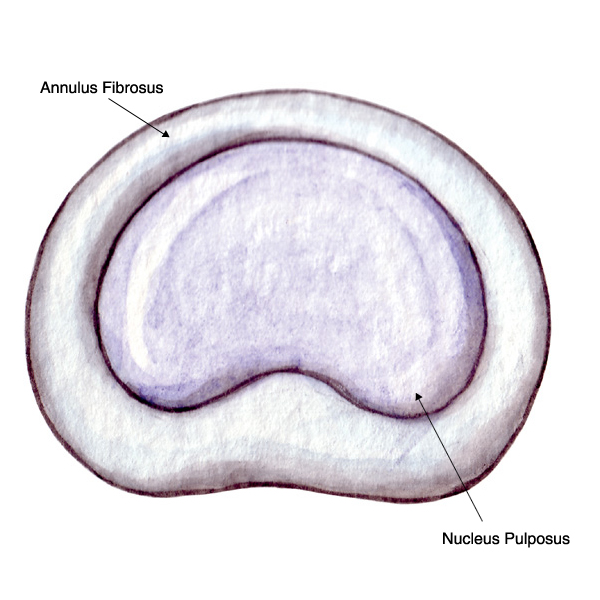
Millions of people suffer neck, shoulder, and arm pain. A herniated disc is a common cause of this pain. Intervertebral discs, which act as the spine’s shock absorbers, are located in between each of the spine’s vertebrae. Each disc contains a tire-like outer band (annulus fibrosus) that surrounds a gel-like substance (nucleus pulposus).
Symptoms
The symptoms of a cervical herniated disc may include:
- Dull or sharp pain in the neck or between the shoulder blades. Pain may be intensified during movement.
- Pain radiating (spreading) down into the arm, hand or fingers. This is called a radiculopathy.
- Numbness or tingling in the shoulder or arm.
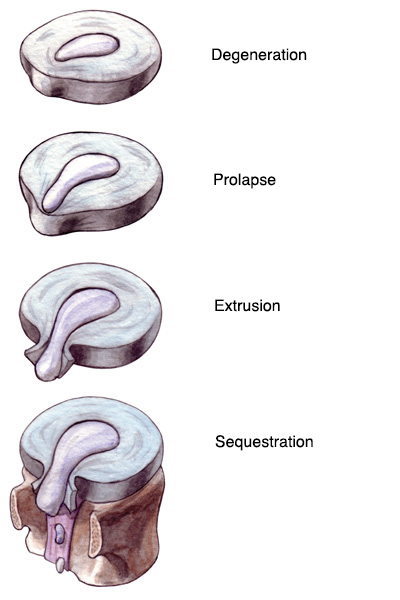
How Discs Herniate
If the disc’s outer band cracks or breaks open, the gel inside the disc can leak out causing a herniated disc. The disc material may place pressure on nearby nerve roots or the spinal cord. Additionally nuclear material releases chemical irritants causing nerve inflammation and pain.
Sudden stress such as from an accident can cause a cervical disc to herniate. Sometimes, a disc herniation develops gradually over weeks or months.
Risk factors that can contribute to disc herniation include:
- Aging. As you get older, discs gradually dry out, affecting disc strength and resiliency.
- History of major or minor cervical spine trauma.
- Lifestyle choices. Lack of regular exercise, eating an unbalanced diet, and tobacco use substantially contribute to poor disc health.
- Poor posture, incorrect and/or repetitive lifting or twisting places additional stress on the cervical spine.
Diagnosis
Cervical disc herniation requires an expert diagnosis, which will include these steps.
- Medical history. The doctor will inquire about symptoms, their severity, and any prior treatments and their results.
- Physical examination. The physical examination includes observations of movement limitations, balance problems, and pain. During the exam, the physician will test the reflexes at the extremities and evaluate muscle weakness, loss of sensation, and signs of possible neurological problems.
- Diagnostic tests. Radiography (X-rays) may be required to observe the cervical spine. CT scans and MRIs may be required.
Nonoperative Treatment
Most cases of cervical disc herniation do not require surgery. Many different nonsurgical treatments help relieve symptoms. These include:
- Medications, such as an anti-inflammatory drugs to reduce swelling and pain, muscle relaxants to calm spasm, and occasionally narcotic painkillers to alleviate acute pain.
- Cold/heat therapy, especially during the first 24 to 48 hours.
- Spinal injections (i.e. epidural) may help relieve neck and related upper extremity pain.
- Physical therapy, which may include gentle massage, stretching, therapeutic exercise, bracing, or traction to decrease pain and increase function.
- Chiropractic or alternative therapy (i.e. acupuncture).
Physical therapists may also provide education in healthy posture and proper body mechanics.
Surgical Treatment
If nonsurgical treatment is ineffective, surgery may be recommended.
An anterior (from the front) cervical discectomy is the most common surgical procedure to treat a damaged cervical disc. The goal of this procedure is to relieve nerve root or spinal cord pressure by removing part of, or the entire disc.
If the entire disc is removed, the surgeon may perform spinal instrumentation and fusion. Instrumentation and fusion joins two or more vertebrae. Instrumentation (i.e. screws, plates) is combined with fusion (bone graft) to stabilize the spine. Bone graft fills the void left when the disc is removed. There are different types of bone grafts, including bone graft from your body. The surgeon will discuss the best type for you.
Many neck surgical procedures can be performed using minimally invasive techniques. Minimally invasive surgery uses smaller incisions and specialized instruments. Minimally invasive procedures benefit you in many ways such as smaller incisions, less time hospitalized, and a faster recovery.
Surgical Recovery
Most patients begin to get out of bed the same day surgery is performed. Activity is gradually increased and patients are typically discharged home within 1 or 2 days after their procedure, depending on the type and extent of the surgery. As with most surgeries, expect some pain after the procedure. Pain medications help keep you comfortable.
At home, continued rest is advised. Patients will be given instructions how to safely and gradually increase activity. Pain medication may be needed for a while. However, pain and discomfort should begin to reduce within a week or two after surgery. Information about other ways to reduce pain and increase flexibility may be provided, along with instructions about when the patient may resume everyday activities and, if appropriate, return to work.
During recovery, patients who make efforts to comply with rehabilitation and learn from physical therapists can develop spine healthy habits for a lifetime that may minimize the risk of future problems.